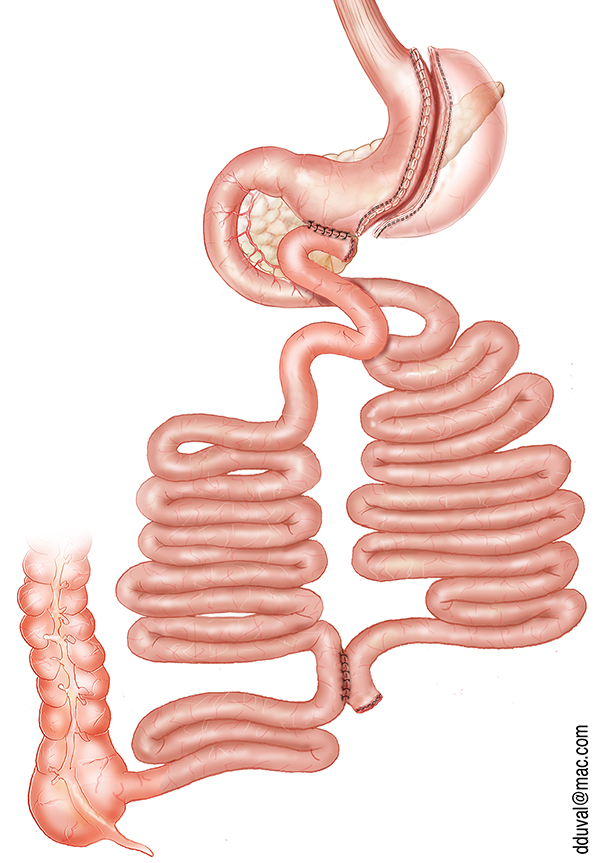
Mini-Bypass

- One anastomosis only
- Reversible
- Cure to diabetes
- Substitution surgery after gastric band failure
- Admission on day of surgery (7am)
- Operating time 45 min
- Drinks allowed the evening following surgery
- Resumption of oral diet the following day with blended foods, to be kept up for 15 days
- Discharge the day after surgery
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol
The Mini-Bypass is the most performed surgery within our team. It has been performed in France since 2005 and has become the alternative to the standard gastric bypass (Roux-en-Y bypass) for 3 reasons :
- its simplicity (1 anastomosis instead of 2 for the Roux-en-Y bypass),
- its efficiency (faster weight loss)
- its reversibility (the mini-bypass can be easily removed, whereas the Roux-en-Y bypass requires a more complex surgery).
Currently, approximately half of the bypass surgeries performed in France are mini-bypass.
Its effect is twofold: restrictive (“I eat less”) and malabsorptive (“I eliminate the fats and sugars that I eat more easily”).
However, the malabsorptive effect favors the emergence of deficiencies, hence the need for lifelong regular follow-ups following this type of procedure. The weight loss is usually complete after 8 to 12 months.
In more than 90% of cases, the mini-bypass also works as a cure for diabetes.
The most common complication following mini-bypass surgery is reflux, which needs to be monitored. Should it becomes too troublesome, please consult your surgeon.

Roux-en-Y Bypass

- Two anastomoses
- Reversible
- Cure to diabetes
- Substitution surgery after sleeve failure
- Admission on day of surgery (7am)
- Operating time 1 hour
- Drinks allowed the evening following surgery
- Resumption of oral diet the following day with blended foods, to be kept up for 15 days
- Discharge the day after surgery
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol
Gastric Roux-en-Y Bypass
In our practice, the Roux-en-Y bypass is an alternative to the mini-bypass. Indeed, it is technically more difficult to perform (2 anastomoses) and the operating time is longer.
We offer the bypass in Y when the mini-bypass is it advisable. Just like the mini-bypass, the Roux-en-Y bypass is both restrictive and malabsorptive. The main complications are vo-miting, dumping, and intestinal obstruction. Weight loss is slower than with a mini-bypass and the risks of vitamin deficiency call for lifelong medical supervision. Technically, it is always possible to remove a Roux-en-Y bypass, though with more difficulty than a mini-bypass. Whatever the type of bypass, diabetes can be cured in more than 90% of cases.

Sleeve

- Resection of 80% of the stomach
- Cannot be reversed
- Risk of acid reflux
- Can be suggested if mini-bypass and Roux-en-Y bypass are not recommended
- Admission on day of surgery (7am)
- Operating time 45 min
- Drinks allowed the evening following sur-gery
- Resumption of oral diet the following day with blended foods, to be kept up for 15 days
- Discharge the day after surgery
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol)
Sleeve Gastrectomy
Sleeve gastrectomy is the second most performed operation within our team. It has also been the most performed operation in France since 2011. The sleeve is purely restrictive ("I eat less so I lose weight"). Historically, the sleeve was the first part of the “duodenal switch” procedure and allowed patients to reach a first weight loss threshold. The surgery consists in resecting about 80% of the volume of the stomach. The sleeve is irreversible and in case of fistula, healing can be difficult. The main complication is reflux. If the reflux becomes too troublesome, the conversion of the sleeve into a Roux-en-Y bypass is always possible. If the patient stills nibbles and has soft drinks after this operation, the risk of weight gain is high. In this case, the conversion into a Roux-en-Y bypass or into a gastric bi-partition (Santoro technique) can be offered after nutritional, dietary and psychological reas-sessments. In some cases, it is possible to perform this procedure by installing a port via transumbi-lical access. This technique, called “single port sleeve”, is purely of aesthetic interest as the patient will have no visible scar contrary to the standard technique (see photos).
Sleeve gastrectomy with transit bipartition (Santoro Technique) (NEW PROCEDURE)

- In case of sleeve failure
- Cure to diabetes
- Duodenum is partially “short-circuited”
- 2 anastomoses
- Reversible
- Admission on day of surgery (7am)
- Operating time 45 min
- Drinks allowed the evening following surgery
- Resumption of oral diet the following day with blended foods, to be kept up for 15 days
- Discharge the day after surgery)
- This pro-cedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] pro-tocol
This surgery is still very rarely performed in France. It was originally described by Dr. Sergio Santoro, a Brazilian surgeon specialised in bariatric surgery. The sleeve gastrectomy with transit bipartition, or Santoro technique, consists in partially excluding the proximal part of the intestine, as opposed to excluding it definitively as is the case in the duodenal switch. This partial exclusion would in theory reduce the risk of vitamin deficiency while encouraging significant weight loss. In a series of more than 1,000 morbidly obese patients operated in Brazil, the results are promising with a loss of excess weight and a cure rate of diabetes comparable to the duodenal switch. This procedure could therefore be an alternative to the bypass and duodenal switch for patients who have already undergone a sleeve gastrectomy and who have regained a lot of weight.