Distal Gastrectomy
- One anastomosis only
- Recommended for cancers of the gastric antrum
- Often coupled with perioperative chemotherapy
- Laparoscopy
- Admission the day before surgery
- No bowel preparation required
- Operating time 1 hour
- Drinks allowed on the evening following surgery
- Resumption of oral diet 2 days after surgery with blended foods, to be kept up for 15 days
- Length of hospital stay 5 days
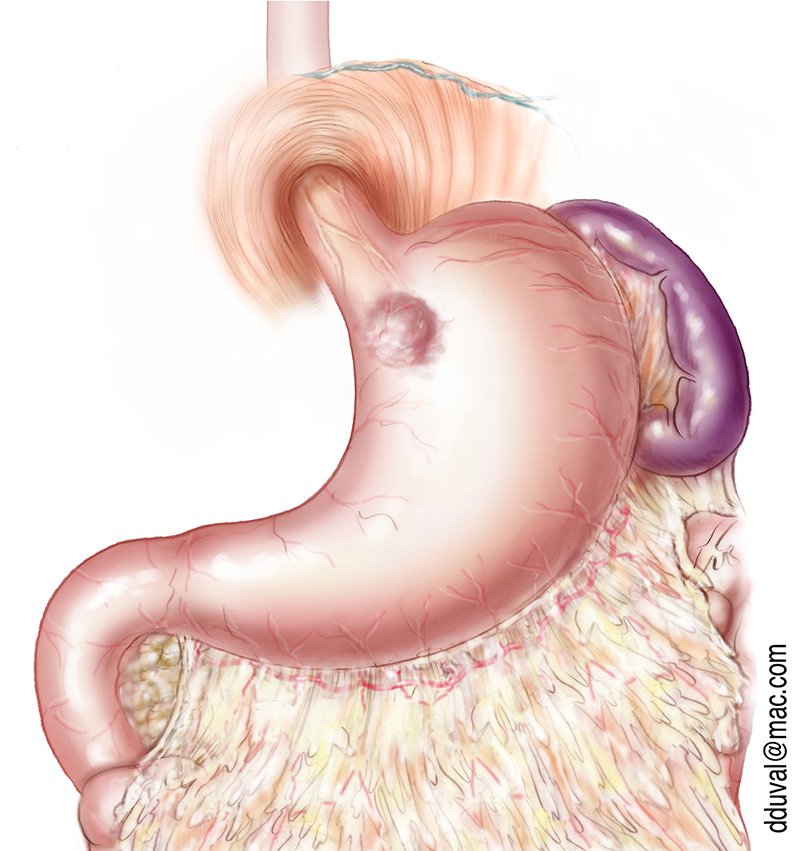
Gastric Adenocarcinoma
The main risk factor is atrophic gastritis (enabled by the presence of the Helicobacter py-lori bacterium).
The first symptoms are chest pains and nausea.
The following tests should be undergone in order to determine the extent of the disease :
- Esophagogastroduodenoscopy, performed by a gastroenterologist
- Thoracoabdominopelvic CT scan, performed in a radiology centre.
Partial gastrectomy under laparoscopy is often recommended when the tumour is located towards the lower part of the stomach, as it offers better functional results than a total gastrectomy. When the tumour is higher, total gastrectomy under laparoscopy is preferred. For locally advanced tumours, chemotherapy is recommended before and after surgery to minimize the risk of relapse.
Total Gastrectomy
- Two anastomoses
- Recommended for adenocarcinomas of the gastric cardia and gastric linitis
- Often coupled with perioperative chemotherapy
- Laparoscopy / admission the day before surgery
- No bowel preparation required
- Operating time 2 hours
- Drinks allowed after 7 days
- Resumption of oral diet 8 days after surgery with blended foods
- Length of hospital stay 10 days
Adenocarcinoma of the Gastric Cardia
This type of tumour is located in the upper part of the stomach, sometimes even on the lower part of the oesophagus. When the tumour invades the oesophageal side, the preferred surgical technique is the Lewis Santi (see section on oesophageal cancer); when it is mostly spread on the gastric side, the most common procedure is a total gastrectomy.
Difficulty in ingesting solid food is usually the first symptom identified.
The following tests should be undergone in order to determine the location of the tumour and its degree of extension :
- Esophagogastroduodenoscopy, performed by a gastroenterologist
- Oesogastroduodenal transit, performed in a radiology centre
- Thoracoabdominopelvic CT scan
If the tumour is operable from the start, chemotherapy is recommended prior to surgery to minimize the risk of relapse. In more advanced forms, radiotherapy can be combined with chemotherapy; depending on the importance of tumour regression, surgery will be considered.
Total gastrectomy can be performed under laparoscopy. It involves removing the whole stomach and rebuilding a “neo-stomach” with the small intestine. Following total gastrectomy, feeding should be portioned to 6 meals per day on average, and an IM injection of vitamin B12 should be given every 3 months.