Atypical Liver Resection

- For small, benign tumours
- Parenchymal sparing
- Laparoscopy
- Admission the day before surgery
- No bowel preparation required
- Length of hospital stay 1 day
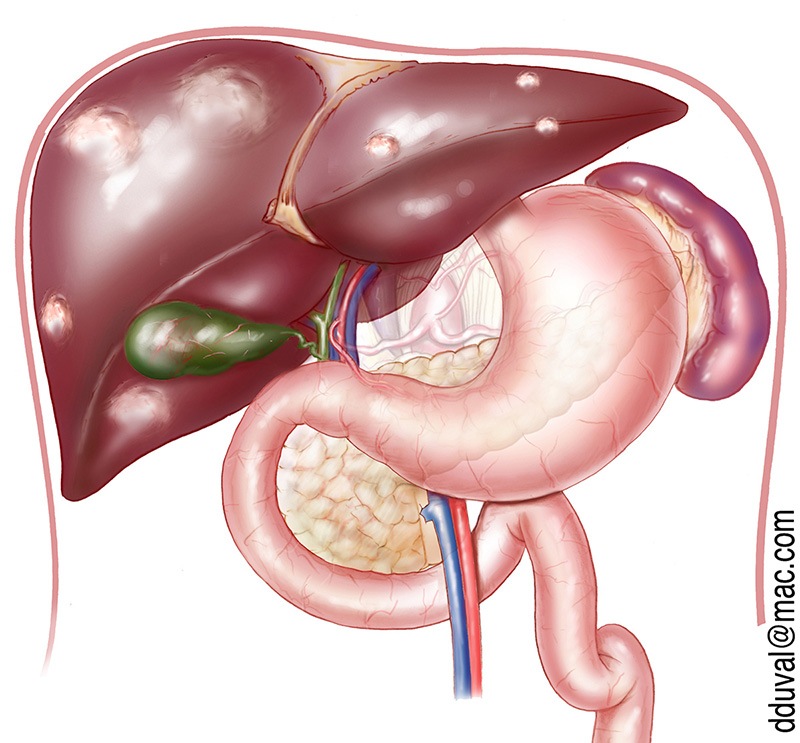
Hepatic Metastases
Colon and rectal cancers hepatic metastases are surgically resectable in about 20% of cases. In other cases, it is necessary to start with chemotherapy to allow a reduction in tumour volume before offering surgery.Surgery is possible if:
- The tumour can be entirely resected
- Preoperative colonoscopy does not show relapse in the colon and/or rectum.
- Chest CT and PET scans do not show pulmonary or bone metastasis
- A good response or stabilization of the disease is observed during preoperative chemotherapy.
It is recommended to consider chemotherapy during the 3 months preceding surgery in order to improve prognosis, even if the tumour is surgically resectable from the start. In cases where resectability is limited or prognosis is hindered by poor factors, preoperative chemothe-rapy gives time to test the aggressiveness of the cancer and its response to treatment; all of which are elements that reflect the tumour biology.
The operation consists in removing the metastases by retaining as much liver parenchyma as possible (Wedge resection). When the tumour is easily accessible, this procedure can be performed under laparoscopy; in other cases, it requires opening. If the tumour is too large, segmental resection is required. Two procedures are possible under laparoscopy:
- left lobectomy (resection of 2 hepatic segments: II-III) for metastases located in the left lobe.
- right hepatectomy (resection of 4 hepatic segments: V-VI-VII-VIII) for metastases localised in the right liver.
After surgery, it is recommended to continue chemotherapy for 3 months, and then mo-nitor: - every 3 months: hepatic function test, tumour marker assay (ACE, CA19-9), hepatic ultraso-nography, lung x-ray.
- every year: colonoscopy & liver scan.